

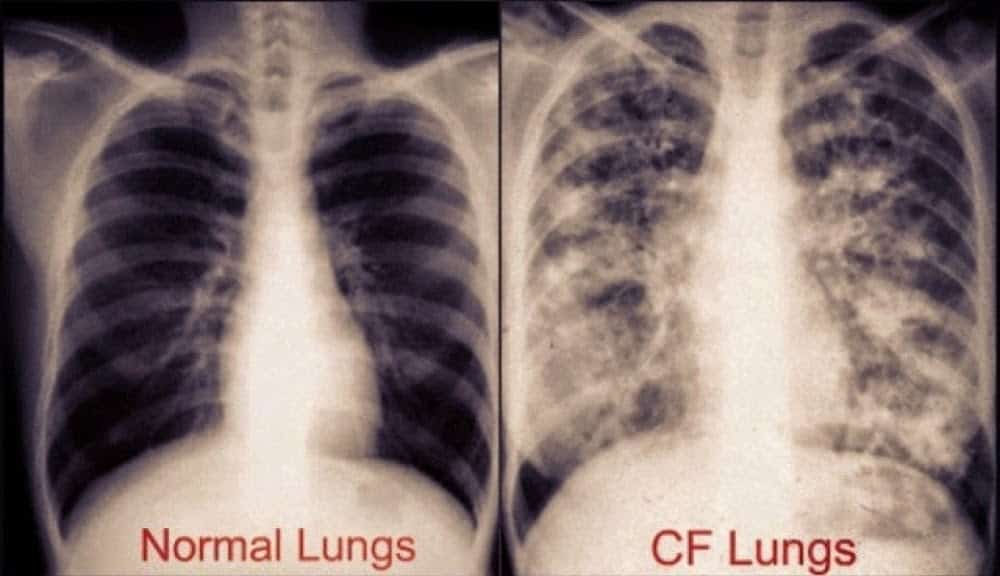
In addition to the primary challenge of compromised lung function, cystic fibrosis (CF) patients are presented with several metabolic hurdles. These issues exacerbate pulmonary symptoms and may be involved with the primary etiology of the disease. There is unequivocal evidence that the majority of cystic fibrosis patients suffer from one form of malnutrition or another (1).
Part of the cause of frequent malnutrition is the decreased production of pancreatic enzymes by CF patients (2). As digestive enzymes in the body decrease, the ability to metabolize and to absorb nutrients is also greatly diminished, particularly with respect to fats, other lipids, and fat-soluble vitamins. This has been reflected in several investigations involving nutritional assessments of CF patients (3,4). On average, Cystic fibrosis patients have altered fatty acid compositions when red blood cell membranes are examined. Increased saturated fat levels and decreased omega 3 fatty acid content reflect an increased reliance on endogenously produced fats as opposed to nutritional augmentation from the diet.
This decreased ability to digest and to properly metabolize fats can be ameliorated by using an enteral formula with ample amounts of omega 3 fatty acids, such as cold-pressed flax seed oil. In addition, it makes sense to utilize a source of protein that requires less pancreatic protease for proper digestion. This would favor brown rice protein or whey protein as opposed to casein, sodium caseinate, soy protein, or milk protein concentrate (MPC), all of which require greater pancreatic exocrine function. Secondary to poor fat absorption, vitamin D levels are also compromised. There are initial reports from a few trials that vitamin D supplementation can improve the lung function and immune response in CF patients (5,6). This is logical, as vitamin D plays such a pivotal role in maintaining both immune function as well as regulating gut wall permeability. As vitamin D levels drop, we would expect to see higher levels of intestinal permeability and an increased susceptibility to lung and upper respiratory infections.
Of equal importance to CF patients is the role of an altered microbiome. This complex ecosystem has an infinite number of influences on lung health, inflammation, microbial translocation-often leading to infected organ systems, as well as overall metabolic capacity. There is consistent evidence that individuals with CF have altered microbiomes with frequent overgrowths of pathogenic bacteria and bacterial overgrowth of the small intestine (SIBO) (7,8,9). While it is unclear if this pattern of dysbiosis drives CF or simply occurs in conjunction with other facets of the disease, it is important to acknowledge and treat the unique CF microbiome. This would entail adding support for the development of healthy, commensal bacterial populations that increase n-butyrate production, thereby improving gut wall integrity and reducing its permeability. Fermentable fiber from a variety of vegetables and/or legumes is the most important dietary attribute associated with this. Eliminating all added sugars, especially fructose and fructose-rich ingredients, is also important for reducing the populations of the more common pathogenic species in CF patients. One may consider the use of a probiotic, possibly added to and thoroughly mixed with an appropriate enteral formula, as an additional intervention to facilitate change.
Lastly, and most interesting, is the role that dietary inorganic nitrate might play in lung function of CF patients. Inorganic nitrate is NOT the type used as a food preservative, but the type that occurs NATURALLY in select vegetables. Vegetables such as beets, celery, celeriac, lettuce, mustard greens, among others, contain the most nitrates. These nitrates increase both pulmonary and vasodilation. Although limited to a number of case studies, there have been repeated reports by CF care providers that dietary inorganic nitrate improves pulmonary function. One recent case study in a pediatric CF patient noted that there was a strong and direct relationship between inorganic nitrate consumption and improvements in CF-related symptoms (10). While we continue to learn more about CF support and how we can improve the quality of life experienced by CF patients, it is very clear that various aspects of nutrition are critical. In summary we should choose foods with proteins that are easier to digest, fats that are rich in omega 3 fatty acids, eliminate the use of added sugar, and be sure that there are ample vegetables in the daily diet.
~ John Bagnulo MPH, PhD.
RESOURCES:
1. Barni GC et al. Factors associated with malnutrition in adolescent and adult patients with cystic fibrosis. J. bras. pneumol. vol.43 no.5 São Paulo Sept./Oct. 2017 Epub July 31, 2017.
2. Decreased ability to digest foods because of pancreatic insufficiency: Singh VK, Haupt ME, Geller DE, Hall JA, Quintana Diez PM. Less common etiologies of exocrine pancreatic insufficiency. World Journal of Gastroenterology. 2017;23(39):7059-7076. doi:10.3748/wjg.v23.i39.7059.
3. Moukarzel S. et al. Complex Relation Between Diet and Phospholipid Fatty Acids in Children With Cystic Fibrosis. J Pediatr Gastroenterol Nutr. 2017 Apr;64(4):598-604.
4. Drzymała-Czyż S, Krzyżanowska P, Koletzko B, et al. Determinants of Serum Glycerophospholipid Fatty Acids in Cystic Fibrosis. Tarantino G, ed. International Journal of Molecular Sciences. 2017;18(1):185. doi:10.3390/ijms18010185.
5. Pincikova T et al. Clinical impact of vitamin D treatment in cystic fibrosis: a pilot randomized, controlled trial. Eur J Clin Nutr. 2017 Feb;71(2):203-205. doi: 10.1038/ejcn.2016.259. Epub 2016 Dec 14.
6. Kanhere M et al. Role of vitamin D on gut microbiota in cystic fibrosis. J Steroid Biochem Mol Biol. 2018 Jan;175:82-87. doi: 10.1016/j.jsbmb.2016.11.001. Epub 2016 Nov 3.
7. Shukla SD, Budden KF, Neal R, Hansbro PM. Microbiome effects on immunity, health and disease in the lung. Clinical & Translational Immunology. 2017;6(3):e133-. doi:10.1038/cti.2017.6.
8. Li L. and Somerset S. The clinical significance of the gut microbiota in cystic fibrosis and the potential for dietary therapies. Clin Nutr. 2014 Aug;33(4):571-80. doi: 10.1016/j.clnu.2014.04.004. Epub 2014 Apr 13.
9. Rogers GB, Narkewicz MR, Hoffman LR. The CF Gastrointestinal Microbiome: Structure and Clinical Impact. Pediatric pulmonology. 2016;51(Suppl 44):S35-S44. doi:10.1002/ppul.23544.
10. Kerley CP, Kilbride E, Greally P, Elnazir B. Dietary Nitrate Acutely and Markedly Increased Exhaled Nitric Oxide in a Cystic Fibrosis Case. Clinical Medicine & Research. 2016;14(3-4):151-155. doi:10.3121/cmr.2016.1320.